Overall rates of long term improvement after spinal surgery for severe chronic lower back pain are about two thirds; between 60% and 70%. It varies slightly depending on the type and origin of the pain. That is, whether it is from stenosis associated with leg pain, herniated lumbar discs, often also with radicular/leg pain, or instability/deformity.
I have all of them, and that combination often results in pain which is both crushing and debilitating. Anti-inflammatories and painkillers, even including opiates, which I take sparingly, never remove the pain. It is constant. They do relieve it enough at night for me to get to sleep, though they don’t last through the night, so pain wakes me with a cheery hello early in the morning. This means tiredness and fogginess are becoming an issue.
I have been able to push through this over the last few years. But now pain not only affects what I can do physically, but my mental power to continue to learn and create, and even my will to do so. Everything about me is drained and diminished.
My doctor has suggested consulting with a spinal/orthopaedic surgeon, but I have met and spoken to so many people who had no improvement after spinal surgery, and in some case became far worse, including affecting mobility, that this could only be an absolute last resort.
Maybe the innovation in treatment discussed at the link will offer some hope. If so I may consider it. But real hope lies elsewhere. I wrote a poem about this which I have copied below:
The Narrowing Room
The pain moves in and drowns the hopes in me,
until I lose the thought I meant to hold;
it dims the page, it darkens all I see,
and turns the warmth I loved to fear and cold.
I cannot sit, or stand, or walk for long
before the fire climbs and claims the hour;
it drains the will that shaped my life’s true song,
and leaves me stripped of purpose, stripped of power.
When COVID-19 began to move around the world in early 2020, doctors faced a virus nobody understood, with no known treatments. In that vacuum, two old, cheap, well-known drugs; hydroxychloroquine and ivermectin, became the focus of enormous hope, and later, enormous controversy. This paper discusses why they seemed promising, how that promise fell apart under scrutiny, and what harm followed.
Neither drug was plucked from nowhere. Both offered plausible scientific reasons to be hopeful.
Hydroxychloroquine had been used safely for decades to treat malaria, lupus and rheumatoid arthritis. In laboratory cell cultures, it showed real antiviral activity against SARS-CoV-2, apparently by altering the acidity inside cell compartments in a way that blocked the virus from entering. It also has anti-inflammatory properties, and researchers wondered whether it might dampen the dangerous cytokine storms seen in severe COVID-19. Early in 2020, a small, poorly controlled French study reported rapid viral clearance in patients given hydroxychloroquine with the antibiotic azithromycin. That single unreliable study was amplified enormously by media, social platforms and political figures, and prescribing took off well before proper trials had been completed.
Ivermectin’s story is similar. It is a decades-old, safe and effective anti-parasitic drug, used worldwide against worm infections, scabies and river blindness. In 2020, an Australian laboratory study found that exposing cultured cells to ivermectin produced an approximately 5,000-fold reduction in viral replication. The proposed mechanism involved blocking the transport of viral proteins into the cell nucleus. News of that result travelled fast, and combined with a handful of small, non-randomised clinical reports suggesting benefit, ivermectin was very soon being heavily promoted on social media.
In both cases, the appeal was understandable: these were cheap, familiar, widely available drugs with a plausible biological story and a handful of encouraging early reports. But that combination; a lab result and a small uncontrolled study, have misled medicine and public perception before, and it did so again here.
The problem with laboratory antiviral activity is that it doesn’t tell you what happens in an actual human body. The ivermectin concentration that produced that dramatic result in cell culture was far higher than what standard, safe dosing could ever achieve in the human body. And COVID-19 entry via the human respiratory tract relies on a different viral entry pathway to the one used in the lab cell lines, one that hydroxychloroquine’s mechanism simply doesn’t touch. Elegant and careful test-tube experiments did not translate into clinical benefit.
The real test came from large randomised controlled trials, which, unlike the early observational reports, assign treatment by chance and so aren’t distorted by differences in age, illness severity or timing between patients who happened to get the drug and those who didn’t.
For hydroxychloroquine, the verdict arrived by mid-2020. The UK’s large RECOVERY trial found no difference in 28-day mortality between hydroxychloroquine and standard care, but noted longer hospital stays and a greater chance of needing ventilation in the group treated with hydroxychloroquine. The WHO’s international Solidarity trial found much the same. Both organisations halted their hydroxychloroquine arms, and the US FDA revoked its emergency authorisation. A later meta-analysis of 26 randomised trials covering over 10,000 patients found a small but statistically significant increase in mortality associated with hydroxychloroquine. In other words, treatment with hydroxychloroquine resulted in more deaths, not fewer.
For ivermectin, the picture that emerged was different but just as clear. Several of the early apparently positive studies turned out to have serious data problems, including implausible results and suspected duplication, and even outright faking of data. The strongest benefits came from the most poorly designed trials. When properly conducted, adequately powered trials were run, including the TOGETHER trial and the PRINCIPLE trial, they found no meaningful reduction in hospitalisation, recovery time or death. A comprehensive Cochrane review, the gold standard for evidence synthesis, concluded there was no reliable evidence that ivermectin prevents or treats COVID-19. https://www.cochrane.org/…/CD015017_ivermectin…
Misinformation about proper treatment can cause real harm.
For hydroxychloroquine, the evidence points to genuine harm at doses given to treat COVID-19. It can prolong the heart’s QT interval, raising the risk of dangerous arrhythmias, especially when combined with azithromycin. Trials also recorded higher rates of gastrointestinal upset, low blood sugar and liver problems, and a higher rate of death than for patients treated with recognised anti-viral medication. Beyond individual harm, the surge in off-label prescribing caused real shortages of hydroxychloroquine in malaria-prone areas, and for the lupus and rheumatoid arthritis patients who actually depend on it.
Ivermectin, taken at approved human doses, doesn’t show the same consistent signal of increased mortality. But that doesn’t mean using it against COVID-19 is harmless. Claims on social media led people to take veterinary formulations meant for livestock, in doses far beyond anything tested in humans. Poison control centres recorded a sharp rise in ivermectin toxicity cases, some resulting in serious neurological and respiratory harm, coma, and death. There is no antidote for ivermectin overdose.
There’s a broader harm too, shared by both drugs: opportunity cost. Time and money spent on medicines that don’t work is time not spent on care that does, including antivirals like nirmatrelvir–ritonavir and remdesivir given early to high-risk patients, and supportive care, oxygen and, in severe hospitalised cases, corticosteroids for those who need them. Chasing an ineffective treatment can delay effective ones, and that delay can carry major risks.
None of this means the initial interest in these drugs was irrational or dishonest. Scientists chase plausible leads; that’s how research works. Both drugs deserved a proper look. The real story isn’t that hydroxychloroquine and ivermectin were fraudulent claims. They were tested rigorously, as they should have been, and the rigorous evidence didn’t support them. Hydroxychloroquine appears to carry modest but real risks with no benefit; ivermectin appears to carry little direct risk at proper doses but no meaningful benefit either, alongside a real toxicity danger from misuse.
Following the evidence, rather than the social media posts, is what protects patients.
Anthony Fauci has spent this week back in the headlines, not for a new discovery but for a Senate hearing. Subpoenaed by Senator Rand Paul, who released more than a thousand pages of Fauci’s private pandemic diary beforehand, the 85-year-old physician sat before the Homeland Security and Governmental Affairs Committee and, for the first time in roughly 250 congressional appearances over four decades, invoked his Fifth Amendment right and declined to answer questions.
Paul has since promised a contempt vote. On social media, the hearing reignited claims that have circulated for years: that Fauci engineered a pandemic cover-up, lied to the public, and profited from a manufactured health crisis. Almost none of that holds up against the documented record of his career.
Fauci joined the National Institutes of Health in 1968 and led the National Institute of Allergy and Infectious Diseases (NIAID) from 1984 until his retirement in December 2022, serving under seven presidents of both parties. Under his direction, NIAID grew from a comparatively minor NIH branch into a research institute with an annual budget in the billions of dollars.
His scientific accomplishments predate his public fame by decades. In the late 1960s and 1970s, Fauci’s team at the NIH repurposed cancer chemotherapy drugs to treat several previously fatal inflammatory diseases, including polyarteritis nodosa and granulomatosis with polyangiitis, turning near-certain death sentences into survivable, manageable conditions. This is work that is still valuable and still taught in medical training today.
In the early 1980s he became one of the first prominent scientists to take the HIV/AIDS epidemic seriously. His early relationship with AIDS activists was adversarial; groups like ACT UP accused NIAID of moving too slowly on treatment access, and playwright Larry Kramer famously branded him a murderer in a 1988 open letter.
Fauci’s response was unusual for a federal official. He did not respond with anger or pressure, but met with activists, brought them into the regulatory process, and helped accelerate access to experimental HIV drugs. Many of his former critics later became allies and credit him with helping transform HIV from a near-certain death sentence into a manageable chronic illness. He was one of few physicians willing to work directly with AIDS patients in the early days of the outbreak. He also worked directly with Ebola patients when there was considerable fear and uncertainty about that disease.
His work on HIV/AIDS fed directly into his best-known achievement: as one of the architects of the President’s Emergency Plan for AIDS Relief (PEPFAR), launched by President George W. Bush in 2003, Fauci helped design a program that the U.S. government and independent health agencies credit with saving more than 25 million lives worldwide and preventing millions of infants from being born with HIV. PEPFAR has long enjoyed rare bipartisan support; Bush awarded Fauci the Presidential Medal of Freedom, and Barack Obama later called him a “once-in-a-century public health leader.”
Dr Fauci has been careful not allow politics to interfere with his research, and has consistently maintained positive relationships with leaders on all sides of politics. Colleagues have repeatedly said they never knew how he voted, and he was registered as a political independent throughout his career. Dr Fauci was and is widely regarded by both colleagues and politicians as not only a capable medical practitioner, researcher and administrator, but as person of both compassion and integrity.
Much of this week’s coverage frames Fauci’s diary as proof of a private man who understood the costs of pandemic restrictions while a public-facing version of him denied that any such costs existed. The public record does not match that story.
On CNN in April 2020, Fauci said that starting mitigation measures earlier would logically have saved more lives, and acknowledged significant pushback against any shutdown at all. By May 2020 he was warning on CNBC that staying closed too long risked “irreparable damage.” In a 2024 CBS interview, he said plainly that keeping schools closed for a full year had been a mistake, even as he defended the initial closures. He did not, in other words, present pandemic policy as costless, but acknowledged social and financial costs in public, repeatedly, over several years.
Separately, diary entries reportedly show Fauci discussing school and business closures with local officials, in apparent tension with his 2024 congressional testimony that he was not involved in local closure decisions. That tension is real and unresolved, and it deserves scrutiny rather than dismissal. It is a narrower, more specific claim than the sweeping “he lied about everything” narrative that has taken hold online, and it is a long way from evidence of criminal wrongdoing or a manufactured pandemic. Diary entries tend more to show a willingness to advise local officials who sought his help, without in any way directing policy.
“He covered up a lab leak.” This is the most serious accusation, and the one driving Senator Paul’s push for prosecution. Fauci has consistently denied that NIAID funded research that created or enhanced the COVID-19 virus, and has pointed to a February 2020 email in which he urged that any legitimate evidence of a lab origin be reported to intelligence officials as evidence of his transparency, not concealment.
I have commented before on the scientific consensus on this issue. This includes the World Health Organization’s 2025 scientific advisory group review, which holds that the evidence more strongly favours a natural, zoonotic origin, while acknowledging that key data from China remains unavailable and that a lab-related origin cannot be fully excluded. U.S. intelligence agencies are divided on the question. Disagreement among scientists in February 2020, three weeks into a novel outbreak, is what the scientific process looks like. It is not evidence of a cover-up.
“Pleading the Fifth proves he’s guilty.” Legal experts note that invoking the Fifth Amendment is standard advice whenever there is a realistic threat of prosecution, and is not itself evidence of wrongdoing. Fauci received a broad, pre-emptive pardon from President Biden in January 2025, but that pardon does not cover conduct outside its window or new exposure created by testifying.
As I mentioned earlier, Dr Fauci has appeared before Congress some 250 times over four decades and has never previously refused to answer questions. Some of the matters raised may give a clue why he was advised not to do so on this occasion, and suggest that Rand Paul’s Senate committee was not conducting a genuine attempt to gain information about COVID research, practice and policy.
“He lied about masks.” Fauci did tell the public in March 2020 not to buy masks, then reversed that guidance within weeks. He and former colleagues have since acknowledged the communication was poor. The reasoning at the time; thin evidence for community masking, a belief that asymptomatic spread was rare, and perhaps most importantly, a critical shortage of protective equipment for healthcare workers, reflected a genuine, if flawed, scientific understanding of an unfamiliar virus in its first weeks, not a deliberate deception. The guidance changed again as the virus and the evidence changed, including clearer evidence of the effectiveness of masks in community settings, and the onset of the more transmissible Delta variant in 2021. Changing advice on the basis of evidence is how science works.
“He pushed an experimental gene therapy that killed thousands.” The mRNA COVID-19 vaccines are not gene therapy, nor were they experimental: they deliver a temporary set of instructions that the body’s own cells use to build a harmless viral protein and then discard, without altering a person’s DNA. Claims of mass vaccine deaths circulating on social media are not supported by any of the extensive safety monitoring systems conducted by the FDA, CDC, and international regulators. Fauci advocated for the vaccines’ rapid development and distribution as NIAID director, and later as the White House’s chief medical adviser, encouraged work that built directly on decades of NIH-funded mRNA and coronavirus research.
“He did it for fame and money.” Fauci’s diary entries do show a man clearly aware of, and at times visibly pleased by, his own celebrity; perhaps a fair target for criticism of his temperament. But being surprised at and enjoying attention and noting this in what were private diaries, may at worst be a character fault, not a corruption charge. It is a considerable distance from the allegations of financial fraud or an orchestrated “coup” against democratic government made in some of the more extreme social media commentary and in Robert F. Kennedy Jr.’s book about him, and for which there is no evidence whatever. Dr Fauci made no money from coronavirus research or from vaccines. He was a salaried public servant, and was in the same position, director of NIAID, for thirty-eight years.
None of this makes Fauci flawless. He has acknowledged real communication failures, particularly on masks. He was, by the account of former deputies and colleagues, a demanding and sometimes volatile boss. Reasonable people can still debate whether U.S. pandemic policy struck the right balance between limiting the virus’s spread and limiting the damage to children’s education and the economy. That is a debate I will not address here, except to note that the evidence available so far, including the widely misquoted University of Chicago mobility studies, still appears too limited to arrive at a definitive answer.
What the documented record does not support is the version of Fauci circulating on social media: a man who secretly engineered a pandemic, knowingly lied about a cover-up, and grew rich and famous off manufactured suffering. Nor does it support claims he visited the Wuhan lab and funded research there, or that he conducted research involving the torture of puppies, or targeted and undermined physicians who disagreed with him, or that he funded and supported research grafting aborted baby tissues into mice. Those claims are false, and the picture of him they create is a caricature.
Set against that caricature is a career that includes curing diseases once considered fatal, helping build the infrastructure that turned HIV into a survivable illness, co-architecting a program credited with saving more than 25 million lives, working through a pandemic in which he became one of the most threatened public servants in modern American history, continuing to show up when subpoenaed when retired and at 85 years of age.
Dr Fauci’s diary entries do not confirm the accusations made by Senator Paul and those he gathered for what seemed more like a scene from The Crucible than a credible investigation. Fauci has a record of more than forty years of public service which resulted in multiple new treatments and programmes which have cumulatively saved millions of lives. He may not be perfect – no one is. But at 85 years of age he deserves recognition and thanks, not false witness, conceit and calumny.
There are two scientifically credible explanations for how the COVID-19 pandemic began (deliberate bioweapon creation is not one of them; there is zero evidence to support that claim, and no experts or credible politicians accept it):
1 Zoonotic spillover. This means that the virus jumped from an animal host to humans, probably at or near the Huanan Seafood Wholesale Market in Wuhan.
2 Lab leak. This is the claim that the virus escaped from the Wuhan Institute of Virology (WIV), sometimes just called the Wuhan Lab.
Evidence favouring zoonotic spillover:
● Market-linked case clustering: The earliest known COVID-19 cases, including many with no direct link to the market, clustered tightly around the Huanan market, and environmental swabs from stalls known to sell live mammals susceptible to coronaviruses tested positive for the virus. Detailed spatial and genomic analyses supporting this were published by Worobey et al., Science (2022) and Pekar et al., Science (2022).
● Two early lineages at the market: genomic work indicates at least two distinct early SARS-CoV-2 lineages (A and B) were circulating, consistent with more than one spillover event from an infected animal pool rather than a single lab escape.
● Precedent: both SARS-CoV-1 (2002) and MERS emerged from animal reservoirs (civets and camels, respectively) via the wildlife trade, giving spillover a strong and recent prior history.
● Virological plausibility: coronaviruses closely related to SARS-CoV-2 circulate in bats across Southeast Asia, and serological studies show some regional human populations already carry antibodies to bat sarbecoviruses (the subset of coronaviruses that includes SARS and COVID-19), demonstrating that bat-to-human spillover is not unusual.
● Genomic features fit natural evolution: analyses have found no clear signature of genetic engineering, and none of the laboratory-adaptation markers (such as mouse-adaptation mutations) expected if the virus had been extensively passaged in cell culture before emerging.
● None of the viruses records indicate were under investigation at the Wuhan Lab could qualify as a predecessor to the early A and B variants of COVID-19.
● The 2025 WHO SAGO report: after roughly 3.5 years of work, the WHO’s Scientific Advisory Group for the Origins of Novel Pathogens (SAGO) concluded in its June 2025 report that the weight of available evidence points to zoonotic spillover, directly from bats or via an intermediate host but stopped short of ruling out a lab leak, noting China’s reluctance to hand over complete information. A summary by 23 of the panel’s members appeared in Nature.
Evidence favouring a lab leak:
● Geographic coincidence: the WIV, one of the world’s leading centres for bat coronavirus research (including gain-of-function-adjacent work), is located in the same city only a few miles from where the outbreak began.
● Illness among lab staff: reports that before the market cluster was recognised several WIV researchers experienced cold or flu like symptoms, which were later claimed to be possible evidence of COVID-19 infection.
● No confirmed intermediate host: despite extensive searching, no animal at the market or in the wildlife trade has been confirmed as infected with a direct SARS-CoV-2 ancestor virus. This is a gap some scientists argue is unusual if spillover were the source.
● The furin cleavage site: some virologists point out that the furin cleavage site in COVID-19’s spike protein is not seen in closely related bat coronaviruses. This requires further investigation. But furin cleavage occurs naturally in many coronaviruses and most virologists consider this unexceptional.
● Limited transparency: China has not released raw case data, WIV lab notebooks, biosafety records, or details of withdrawn viral-database entries. This is suspicious, and is an obstacle multiple investigators, including WHO’s own SAGO team, say has prevented a conclusive assessment either way.
Where does the preponderance of evidence lean?
There is no definitive, universally accepted proof for either hypothesis. Most virologists and epidemiologists who have studied the case data continue to lean toward zoonotic spillover, centred on the Huanan market, as the better-supported explanation, while a minority of scientists and several intelligence agencies consider a lab-related origin plausible or more likely. The WHO’s 2025 SAGO assessment explicitly kept the question open, noting that missing data from China was the main obstacle to a firm conclusion. The two positions have also become associated with different national and partisan narratives, which has made the scientific debate hard to separate from political issues..
This is a song we wrote based on a suggestion made by Kathy, about the constant demands for hate and outrage on social media.
It was not going to be released for a few months yet – we are working on other projects. But the torrent of hate directed at Anthony Fauci over the last few days prompted a preview on Soundcloud, especially since Fauci is mentioned specifically in the song.
Let’s consider some of claims made about Dr Fauci’s private diaries, made public by Senator Rand Paul:
Dr Fauci covered up his own vaccine injury to hide the dangers.
He didn’t suffer a vaccine injury.
Dr Fauci lied about the case fatality rate, pretending it was between 1% and 2% and that it was ten times more dangerous that seasonal influenza, when it was really closer to 0.1%.
The case fatality rate for COVID-19 IS between 1% and 2%. It is ten times more dangerous than seasonal influenza, not even taking into consideration the serious long-term negative effects of serious COVID infection.
Dr Fauci personally approved research involving the torture of puppies.
Dr Fauci knew the virus had been leaked from the Wuhan lab and covered it up.
He considered the evidence that it had been leaked from the lab, and concluded, along with almost all other virologists and epidemiologists, that this was highly unlikely, and that it had come from the large “wet” markets a few miles away. This is still the evidence-based view held by most researchers. I will write a bit more on this later.
Dr Fauci visited the Wuhan lab with President Obama and Melinda Gates in 2014, and said not long after that there would be pandemic in the USA.
Dr Fauci has never visited the Wuhan Institute of Virology. Claims to the contrary are based on a photo passed around social media. That photo was taken at National Institutes of Health (NIH) Vaccine Research Center in Bethesda, Maryland, USA. The woman claimed to be Melinda Gates is not Melinda Gates but Sylvia Burwell, who was then serving as the U.S. Secretary of Health and Human Services. Fauci did not say there would be a pandemic in the USA as if referring to a specific event. He and other researchers warned frequently and over a long period of time that a large scale pandemic was inevitable, and that ongoing research into infectious diseases was essential to ensuring public safety.
Simply, don’t repost demands to hate, or posts that encourage outrage. If you don’t know something is true, don’t post it.
Low budget movie Citizen Vigilante has been a huge success over the last two weeks, in part because of Germany’s decision to ban the film from screening, and Elon Musk’s subsequent decision to make it available to view free of charge on X, formerly known as Twitter.
Rotten Tomatoes is usually a reliable guide to movie quality, because it balances critic reviews against large numbers of viewer reviews. The viewer reviews are usually better. In the case of Citizen Vigilante, the critic score is zero, while the viewer score is 94%.
Technically, Citizen Vigilante is not a bad movie. Uwe Boll’s direction is crisp and fast-moving. Armie Hammer as the protagonist Sanders is consistent, compelling and frightening. The movie starts fast, and does not let up. It is continuously, if dismayingly, engaging.
Nonetheless, I understand the critics’ concerns, and Germany’s decision not to allow public viewing.
Communities in Western nations which have welcomed large numbers of immigrants from cultures with values and practices substantially different from our own have genuine reasons to feel anxious: reports of large increases in violent crime, sexual assault, strained policing, and court sentences that are too lenient to deter offenders or satisfy victims.
These frustrations are genuine, and Citizen Vigilante trades on them.
But Citizen Vigilante is not a redemptive power fantasy. It is not about redemption or justice at all. Its protagonist is not a good man pushed past his limits. He is a psychopath, and the film, or at least a large majority of its viewers, mistake his pathology for heroism.
The evidence of this is what Sanders actually does. He kills people who simply get in his way. He kills to make a point, staging violence as theatre rather than as a last resort. He treats women as objects for his own amusement and pleasure, not as people. The scene in the brothel is horrifying in a different way from the rest of the movie, but it demonstrates the same inability or unwillingness to see and treat others as fully human
The crime victims he claims to avenge are barely characters at all; they exist only as a pretext, as props whose suffering justifies his next kill. A story genuinely about justice would be centred on the victims’ needs. This one uses victims and discards them.
That distinction matters, because it exposes the trick at the heart of the vigilante myth. When institutions look paralysed, the lone avenger seems purifying: unburdened by paperwork, due process, or restraint. Citizen Vigilante invites us to conflate frustration with justification; to feel the protagonist’s anger and mistake that feeling for endorsement.
But a man who murders for convenience and spectacle, for his own satisfaction, is not motivated by justice. His grievance is a costume.
Strip away that costume and the vigilante’s central flaw stands out: an absolute belief in his own infallibility. He is investigator, jury, judge, and executioner, with no check on his judgment and no accountability for his errors. This flaw is fatal to long-term stable society. Vengeance of this kind is not a purer form of justice; it is not even justice with the safeguards removed. It is not justice at all. Because he cannot guarantee the accuracy of his targets or the proportionality of his response, Sanders becomes the danger to public safety he claims to be eliminating.
Nor does his violence stay contained, limited to those who have committed grave crimes. Vigilante action doesn’t restore order, it accelerates disorder. Every act of summary violence invites retaliation, arms rivals, and forces police to spend their time containing freelance warfare instead of investigating crime. The result isn’t a safer street; it’s a theatre of conflict where bystanders get caught in the crossfire, and where fear, not law or a sense of mutual obligation, is what makes people fall in line.
The deepest damage is to the social contract itself. Courts can be frustratingly lenient, and institutions can feel slow and unresponsive. These are real problems requiring reform, engagement, and public pressure. Vigilantism offers a shortcut that destroys the machine instead of fixing it.
Once the protagonist acts with impunity, he sends a message that personal judgment outranks codified law. If everyone accepts that logic the only question left is who has the bigger gun. That is not, and cannot be, justice. Nor can it lead to a safer, more trusting society. It is a return to tribal violence as in Hutu vs Tutsi. It also provides a ready-made blueprint for anyone with a grievance to claim his or her violence is righteous, or at least, righteous enough.
Real heroism, and real justice, look nothing like this. They are slower and less cinematic. They demand institutional accountability, support victims as people rather than plot devices, and do the patient work of civic repair. Citizen Vigilante dresses up a psychopath’s appetite for violence as a solution to a broken system. Sanders is not the model of a cure for that system’s failures. He is a symptom of something just as dangerous.
In June 2026, outgoing US Director of National Intelligence Tulsi Gabbard released declassified documents which she claimed implicate Dr Anthony Fauci in the origins of the COVID pandemic.
Specifically, she alleged:
• Dr Fauci knowingly funded gain of function research at the Wuhan Institute of Virology (WIV) resulting in the creation & subsequent leak of COVID-19
• Dr Fauci manipulated intelligence assessments to conceal his involvement
• Dr Fauci lied to Congress
• Dr Fauci used a ‘Deep State playbook’ to suppress dissent among his peers
The documents Gabbard linked to as support for these claims instead disprove her allegations.
The National Institutes of Health (NIH) funded coronavirus research at EcoHealth Alliance (EHA), an American non-profit organisation that studies emerging diseases. EHA was partnered with the WIV (& others) for the study of coronaviruses in China. Money from the NIH grant was directed to the WIV via EHA.
Dr Fauci was Director of the National Institute of Allergy & Infectious Diseases at the time, not the NIH. He was not personally responsible for the allocation & oversight of research funding (the NIH grant process is a complex one, conducted via multiple committees, not one person). He had no oversight or involvement the administration of EcoHealth Alliance.
There is no evidence that US-funded work created COVID-19. There is no evidence that viruses studied under NIH/EcoHealth funding could have evolved into SARS-CoV-2.
Gabbard cites documents & internal communications from the National Institute of Allergy & Infectious Diseases (NIAID) in support of her claim that Dr Fauci pushed the intelligence community (IC) ‘to endorse a natural, animal origin to hide his dangerous research.’
Those documents exonerate him & contradict her.
Dr Fauci took an interest in intelligence briefings, but did not hand pick the staff responsible, did not steer an intelligence assessment and was kept at arm’s length by the IC.
Gabbard misrepresents Dr Fauci’s June 2024 testimony to the House Select Subcommittee on the Coronavirus Pandemic, in which he corrects the misapprehension that he had no communication with the IC during the pandemic. On the contrary, he clearly states that he was briefed by intelligence agencies about possible lab activity after COVID origin investigations began.
Gabbard accuses Dr Fauci of ‘lies, disinformation & censorship’ as part of a wider scheme to shield himself from scrutiny while maintaining his influence. The documents she cites show the opposite.
Dr Fauci has testified before Congress on numerous occasions, and endured relentless scrutiny from lawmakers and the press. There is no evidence he pressured or censored any of his staff, or anyone in the intelligence community.
This is a reply to a post on a “pro-science” social media page. That page is a good source of information, but also leans towards being anti-Christian, mainly because its view of Christianity has largely been shaped by American fundamentalism, now sadly and widely exported to Australia and New Zealand. ———————————— The following claim is not accurate: “Galileo Galilei was forced by the Catholic Church to abjure his evidence-based conclusion that the Earth revolved around the sun, which contradicted the literal interpretation of scripture. At the time, the church considered the literal Biblical word immutable, and suggesting otherwise was heresy.”
There was no compelling evidence for the heliocentric theory at that time, and the mathematics to make it work were more complicated than for geo-centrism. Kepler’s theory of elliptical orbits fixed this problem, but that still did not amount to anything approaching proof.
Heliocentrism was widely taught. No one had an issue with it as a theory (I do not mean theory in the sense of evolutionary theory or gravity here, but in its common sense as something unproven). Its status as a theory – an unproven possibility – was all that was justified at that time.
Nor did the Church at that time hold to a “literal and immutable” understanding of Scripture. That, in the sense of modern fundamentalism, is a far more recent invention. The Church had always recognised and understood that the Bible includes multiple different forms of literature, and that these need to be interpreted carefully, prayerfully, and in accordance with their history and genre.
1,000 years before Galileo, St Augustine had said that the facts about the world and its origins can be known “with the greatest certainty by reasoning or by experience,” even by non-Christians, and that Christians should avoid contradicting the findings of science when interpreting Genesis. He also said it is “disgraceful and dangerous” for a Christian to talk foolishly about these matters while claiming to explain Holy Scripture.
Cardinal Bellarmine, the Cardinal in charge of the enquiry into Galileo and his fitness to hold a teaching position, wrote in 1615 that if a proven natural truth appeared to make any interpretation of Scripture false, we should be willing to consider that it was our interpretation that was incorrect, and try to do better. In his own words: “No effect of nature established by experience or necessary demonstration should be made doubtful by Scripture passages that admit multiple interpretations.”
Galileo refused to teach anything except his own pet theories. In many of these, he was completely wrong. For example, as Einstein noted in 1953, Galileo’s theories about tidal action were nonsense. Galileo believed the rings of Saturn were not rings but a large moon on either side. He was savage in his attacks on Jesuit astronomer Orazio Grazzi, who correctly described comets as small heavenly bodies, while Galileo insisted they were reflections shining on vapours rising from the earth. In each of these instances, Galileo refused to teach or consider any other possibility.
The disagreement was not primarily about heliocentrism, or about the interpretation of Scripture. It was about Galileo’s persistent refusal to teach anything except his own views. Instead, the Church insisted, on matters which could not absolutely be proven one way or another, that every reasonable possibility should be presented, evidence for each offered and argued, and students permitted to arrive at their own views (which they would then be required to defend) based on the evidence.
This why Feyerabend noted that during that dispute the Church in its argument and attitude was far more reasonable and science-friendly than Galileo. It is an argument and attitude from which many contemporary learning institutions would greatly benefit!
Cardinal McElroy recently claimed that the Church needed to pay more attention to “the lived experience” of LGBTQIA2S+ people, and be accepting of who they are, and therefore, of what they do.
I disagree.
I have spent a considerable amount of time in prison ministry. Much of this has been spent in protection prisons. The largest cohort in those prisons is sex offenders. Many of the claims for tolerance, support and celebration made by LGBTQIA2S+ people are also made by paedophiles. I use that term in its technical meaning, which refers to persons whose primary or only sex drive is towards pre-adolescent children.
Some child sex offenders are very much aware of the abhorrent and immoral nature of adult-child sexual interaction, and the long-term harm it can do. They struggle constantly with feelings and urges which they did not choose, and over which they have no control. Many of those I spoke to had offended only once, and felt deep and genuine shame. Many of them had repeated bouts of suicidality. Paedophiles have a suicide rate fifteen times higher than the general population.
I was never judgemental of them as people. If my only sexual drive was in a direction forbidden by society, would I be strong enough to go my entire life without any expression of that sexuality? I hope so. I’d like to think so. But I know myself well enough to know that it would be a constant and painful struggle.
But understanding, or trying to understand, their struggle, and even their failures, and bringing hope of healing and redemption in Christ did not, does not, and cannot mean accepting or affirming their right to act on their impulses, no matter how strong or how natural or how innate those impulses seem to them to be.
Others with that same attraction do not apologise for their feelings, or for “who they are.” They were made this way, they claim, so this is the way they are meant to be. This is their lived experience. In Australia, this advocacy has taken the form of groups like BLAZE and Child Liberation. Children, they claim, are sexual beings, and exploring that sexuality is an important part of discovering who they are and how they relate to the world. Refusing to allow children to explore that sexuality in a safe way, perhaps with caring and responsible adults, is not about protecting children, but about protecting our ideation of childhood as innocent and asexual. It is modern society, not paedophiles, who objectify and abuse children by denying them the right to be who they are, and to explore who they are in a safe and inclusive way.
Those who take that point of view draw on the work of academics like Edward Brongersma, who argued that adult-child sexual interaction had no intrinsic long-term negative outcomes and that it was almost inevitably the secondary intervention by alarmist and judgemental parents, police, and social workers which caused the harm.
Theological arguments have also been drawn in support. Peter Lineham is a New Zealand historian and theologian who has been vocal in support of LGBTQIA2S+ people. His argument is that people on those spectrums did not choose to be who they are. Whether they were “born that way” or their sexuality developed over a period of time is irrelevant. The direction of their sexuality was not chosen; it is intrinsic, experienced as a given.
Mr Lineham goes on to say that Christians believe in an infinitely loving, infinitely inclusive God. It is simply not possible, he says, for Christians to believe that such a God would create people with these deeply felt urges, which they experience as part of their identity, and then condemn them for acting on those urges. We must, he says, listen and learn from their lived experience. We must accept them, and celebrate their givenness as we do our own.
Such arguments are immensely appealing to paedophiles, who also experience their sexuality as something they did not choose, as part of their givenness, as part of who they are. A just and listening society, they claim, would join with them in celebrating their identity.
We do not accept this in relation to that cohort. We should be cautious in accepting it in relation to others. An essential part of Christian theology is the Fall. The world is not the way God intended. Sin undermines, infects, and affects all of creation, everything we do, and how we perceive ourselves.
It is true, as Cardinal McElroy points out, that sexual sins seem to receive a disproportionate amount of attention from the Church, although the extent of this attention is often exaggerated. The Church’s demands for peace and justice and care for the environment are less controversial, and therefore less newsworthy.
There are two reasons for this attention to sexual sin that the Cardinal does not mention.
Firstly, there is no other group of sins which we are lobbied to accept and even celebrate. We do not have a month to celebrate envy, although it could be argued that TV advertising has made this a permanent celebration. We do not have campaigns to normalise abuse of parents, or demands that theft be recognised as a normal part of human nature.
Where a society has gone deeply astray from life and does not recognise that fault, that is where it will most feel the Church’s demands for truth and virtue as oppression and injustice. Of course, the Church’s teachings on morality apply only to Christians, who have a new identity in Jesus, and who above all should be seeking to live humbly, justly, and in accordance with God’s will.
Secondly, the Church spends some time on sexual sins because there is no other family of sinfulness that is so deeply embedded in us that it is perceived as part of who we are. I suffer the same besetting or habitual sin as St Jerome, although I do not go as far as hitting myself on the head with a rock every time I fail. We perceive other sins as something to be acknowledged and resisted, even if we fall regularly. It is only in the area of sexual sins that society encourages us to be free, to express ourselves as we truly are, to see that sin not as sin but as an inescapable and given part of our identity. This is a view the Church, and we as individual Christians, must persist in rejecting.
Careful listening and compassionate acceptance of people’s lived experiences will take us towards understanding, forgiveness, and acceptance of ourselves and of others whose sins we do not understand. It will even lead us to love for people regarded as unlovable, as beyond the pale of forgiveness and acceptance, because we are called to love as Jesus loves.
What deep listening to lived experience cannot do, and must not do, is lead to acceptance of sin itself, to acceptance of the idea that any sinfulness, including my bad-temperedness, is to be celebrated, lived with, and accepted.
Anti-vax and anti-science posters on social media often ask questions to which they absolutely do not want answers.
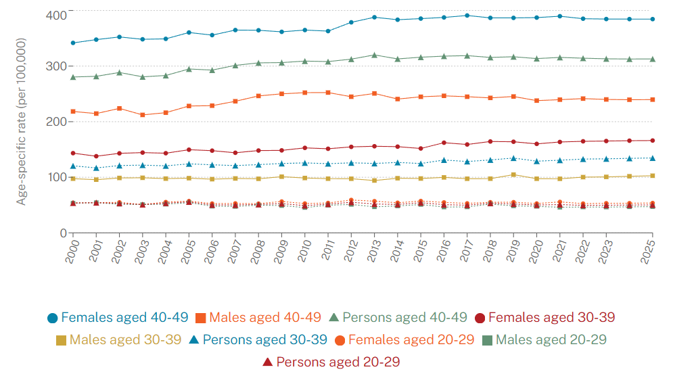
For example: If you think the government cares about you, why don’t they care about the massive increase in cancers in young people? No one has any answers!
Let’s quantify “massive” for a start. Cancer diagnoses amongst people between 20 and 29 increased from about 2.2 per 100,000 population to about 4.6 per 100,000 population in 2025. That is certainly a statistically significant figure, but “massive” is an alarmist exaggeration.
The data commonly cited as showing increases in cancer rates in young people dates from between 1999 and 2020. It cannot have anything to do with COVID vaccines, which were first rolled out in Australia in February 2021.
In research and medical circles, as opposed to social media, the reasons for the increase in the number of cases diagnosed are well-understood. Firstly, increased, earlier, and more precise diagnostics mean we are catching more cancers earlier. Not that they weren’t there before, we are just doing a better job of finding them.
Obesity, sedentary lifestyles and occupations (far more people now spend their working days sitting in a chair), processed foods and alcohol consumption also have a role.
You can reduce your risk by taking some simple steps. Don’t smoke or vape. Exercise regularly. Stay close your ideal weight. If you consume alcohol, do so only occasionally and in small amounts. Reduce intake of heavily processed foods. If your job is largely sedentary, get up and walk or do some stretches every half hour.
In addition, it is worth remembering average lifespan is longer than thirty years ago, and cancer is highly correlated with higher age. While not related to incidence in younger people, this means we would expect to see higher rates of cancer simply because people are living longer.
Old or young, the key thing to remember is that even though more people are being diagnosed with cancer, fewer people are dying of cancer. We are, very gradually, beating cancer back.
Over the last two weeks I have read through the Brereton report, Justice Besanko’s judgement in Roberts-Smith v Fairfax Media, the judgement of the Federal Court in Roberts-Smith’s appeal, and both Crossing the Line: The inside story of murder, lies and a fallen hero (2023) by Nick McKenzie, and Flawed Hero: Truth, Lies and War Crimes (2023) by Chris Masters.
This was no trivial undertaking, amounting to well over 2,000 pages of careful reading. I did this because I continue to see on social media comments on this case which are, to say the least, ill-informed.
For example, the claim that Andrew Hastie was BRS’s commanding officer and therefore should be charged too, if anything wrong was done. Hastie was never at any time BRS’s commanding officer. Or the claim that armchair critics should not judge decisions made in the heat of battle. That is true as a general principle, but has no application in this case. None of the charges relate to actions taken in battle. Or the claim that Australian Federal Police and Federal Courts have no jurisdiction to hear military matters. That is simply false.
This has become a matter of national interest, in part at least because it reflects on our national character.
The claims made by many of BRS’s fellows in the SASR, are, if true, a shocking indictment of a very few who betrayed their companions, their regiment, the people of Australia who trusted them to act in their name, and the people of Afghanistan, whom they were there to protect from Taliban terrorists and to assist in the establishment of a long-term viable democratic government.
We have an obligation to investigate and deal honestly with credible accusations of war crimes involving Australian service men and women. This is not just a matter of law, including international law relating to conduct in war to which we are parties, but a matter of integrity, of simple right and wrong.
I will give a quick overview of each of the documents listed above.
The Brereton Report, about 460 pages, gives useful background. What constitutes a war crime. What provisions exist in Australian and International law to investigate and prosecute allegations of such crimes. How Australia has acted in the past in relation to claims of war crimes committed by Australian forces. But matters concerning the specifics of issues of current concern have been heavily redacted, removing names, dates, and locations. This makes it difficult, though not impossible in a few instances, to identify people or incidents referred to. This includes one incident Brereton describes as the most shameful in the history of Australia’s armed forces.
Justice Besanko’s judgement runs to over 700 pages, and is gripping but sometimes difficult reading. This is the judgement in the case claiming defamation Ben Roberts-Smith brought against Fairfax Media, and against Nick Mckenzie and Chris Masters.
I have read several judgements in civil and criminal cases. This is the most detailed and thoroughly argued I have so far encountered. It is an extremely careful and fair-minded consideration of multiple strands of evidence – Sametime Chat records, satellite and GPS evidence, Operational Summaries, photographs, flight and military personnel records, along with evidence given by dozens of witnesses. It is, in the end, compelling.
The judgement of the Full Federal Court in the Appeal is shorter, just over 200 pages. It is a response to issues raised by the applicant in which he suggests Justice Besanko failed to consider evidence, or failed to take exculpatory evidence appropriately into account. The applicant’s claims are considered in detail, and where necessary, witness testimony and other evidence reviewed. The applicant’s submissions were rejected, with explanations given of the Court’s reasoning in each instance. This document provides some useful clarification of the timeline of some key incidents.
The books by Nick Mckenzie and Chris Masters are both well-written and continuously engaging. Nick Mckenzie’s book is more personal. At times his descriptions of the impact on Afghan families of mistreatment by Australian soldiers, including the murder of family members, are deeply moving. So are his descriptions of the impact of such actions on the mostly decent soldiers who observed them.
Chris Master’s book is a more objective history of how initial rumours were investigated and how investigations interacted, leading to long-lasting military inquiries, media reports, and eventually to the trial, instituted by Roberts-Smith, at which it was found on the balance of probabilities, to Briginshaw standards, that he had tortured, murdered, and incited the murder of non-combatants.
It may be difficult reading, especially if you have no legal background, or if you do not have a high level of reasoning and English comprehension skills.
Then read one of the two books mentioned above. Both give a good summary of events leading up to the trial.
Having read all that, you will still not be entitled to come to a conclusion about Ben Roberts-Smith’s guilt or innocence. I do not regard myself as being entitled to do so.
The standard required for conviction of a criminal offence is much higher than in a civil matter. It is sometimes described as “beyond reasonable doubt.” What this means is that if there is any reasonable explanation of all the evidence, taken together, which is compatible with defendant’s being innocent, then a verdict of Not Guilty must be returned.
The question then is: “Are there any instances amongst the matters with which BRS is charged, for which no other reasonable explanation of the evidence can be found except that he acted as charged.” And that is for a jury to decide.
Nothing is “free,” obviously. Free just means someone else is paying for it. Sometimes that may be justified, but there is nothing intrinsically virtuous about the government taking people’s money and giving it to someone else.
The other issue with “free,” is that free always costs more, whether it is education, health, or nappies. A perfect example is the free diapers to be given to parents of newborns in California. Lovely idea. Why not help out?
Well, first, because it is someone else’s money, someone who has worked for it and may be in just as much need as the new parents.
And secondly, because because the free diapers cost taxpayers at least three times more than if the parents had bought them themselves.
As the article linked below points out, if the government really wanted to help, a much more efficient way to do so would be to give parents a voucher they could spend at a local retailer. Or even better, stop interfering, and just let people pay for what they want according to their own priorities, with money they have earned.
One of the constant refrains from the anti-vax conspiracy crowd during the COVID-19 pandemic was that masks don’t work. “Don’t you know how tiny viruses are? They can easily get through any mask. It’s like trying to stop mosquitos with chicken wire. It’s all about control.”
Could they be right? Did they really notice something that had escaped the attention of surgeons, respiratory physicians, epidemiologists, virologists, and frontline health care workers for the last hundred years? Well, no.
Viruses are very tiny. Much smaller than the gaps in any mask you could breathe through. But as medical researchers and doctors repeatedly pointed out, viruses don’t travel around on their own. They sit in moist or greasy spots on surfaces or float around in droplets of water exhaled in sneezing, laughing, coughing or even just breathing. Inhalation of almost all of those droplets can be prevented by any good respirator or surgical mask.
Researchers learned very early that COVID-19 was not commonly spread through surface contact, but though inhaling infected droplets. Any reduction in initial viral load improves your body’s ability to recognise and respond to infection. So masking should work. Even cloth or paper masks which are less effective may still reduce viral load enough to allow a more robust immune response.
But did they work? Just to be clear, there is no doubt that respirators and surgical masks dramatically reduce the risk of infection in clinical situations. Decades of experience and multiple studies have shown this. The question is, do they have a worthwhile effect in reducing transmission as a population-wide measure?
The answer is yes. In areas of high risk of aerosol/respiratory transmission, masks significantly reduce the risk of infection.
A recent large scale study in the USA compared infection rates in counties which mandated masks in periods of high risk with counties that didn’t, taking into account other factors such as population proximity and age. Mask mandates, even though sometimes unpopular and not fully complied with, resulted in lower rates of infection and death.
Hantaviruses were first isolated in the late 1970s, with Hantaan virus named after the Hantan River, the site of Korean War haemorrhagic fever investigations. Old World hantaviruses (e.g., Hantaan, Puumala, Seoul, Dobrava‑Belgrade) cause haemorrhagic fever with renal syndrome (HFRS), while New World hantaviruses (e.g., Sin Nombre, Andes) cause Hantavirus Pulmonary Syndrome (HPS).
The variant that caused illness and death on the cruise ship MV Hondius is the Andes virus. ANDV is the main cause of HPS in Argentina and is considered endemic but rare, with about 100 confirmed HPS cases per year nationally over many years, concentrated in specific regions such as Andean Patagonia and the northwest.
Most hantaviruses only move from rodents to humans via inhalation of aerosolised rodent excreta, but Andes virus is exceptional in that it can be transmitted between people through close, often household‑level or intimate contact, for example through exhaled droplets (aerosols) especially in the early fever phase, and especially in confined spaces.
One well-known outbreak occurred in Epuyén in Argentina in 2018. A man who had been infected via exposure to rodent excreta attended a birthday party while symptomatic and infected several people. Infection chains extended through family, funerals, and hospital contacts, ultimately giving 34 cases and 11 deaths before strict isolation and contact tracing stopped the outbreak.
Large numbers of cases of HFRS prompted the development of vaccines, which were rolled out as follows:
– 1990s: Inactivated Hantaan/Seoul vaccines are rolled out in China and South Korea, resulting in a large drop in HFRS cases.
– 2000s–2010s: Multiple recombinant, subunit, and DNA vaccine candidates for HFRS and HPS are evaluated, but none are licensed globally.
– Late 2010s–2020s: First Andes virus DNA vaccine reaches human phase 1 and shows good safety and immunogenicity; mRNA and other platforms show strong animal protection but have not yet been fully tested and licensed for human use.
It is likely that the first case in the recent outbreak, a Dutch man who had visited several sites with potentially high native rodent populations, was infected through the inhalation of dust from rat faeces. The infection was then probably – probably only – this has not been confirmed – spread via aerosol droplets to other passengers with whom he was in close contact.
Should we be worried? Not especially. The fatality rate is between thirty and forty percent. Eleven people out of thirty-four known infections in the Epuyen outbreak died. There is no known cure, and at the moment, no approved vaccine. Hantaviruses are found everywhere in the world except Australia and New Zealand. The highest burden of disease occurs in South America and South-East Asia. The Pumala variant is found in Northern and Eastern Europe and causes a less lethal version of HFRS. The Dobrava–Belgrade variant occurs n the Balkans and Western Russia, and causes a much more serious and more often fatal version of HFRS.
But, and it is very big but, the only known variant which spreads between humans is Andes. If you visit areas of South America with high rodent populations, wear a mask and wash your hands carefully after any potential exposure. If you know someone who has recently returned from visiting such areas, and you are going to be in close proximity to that person, observe the same precautions when nearby for a period of a month.
While the consequences of infection are potentially catastrophic, the chances of infection in normal life anywhere outside endemic areas is virtually zero. So be aware but not worried.
What are we to make of some of the anti-vax and conspiracy claims that are being passed around social media? Nothing at all, except that they confirm the gross ignorance of anti-vaxxers, combined with a complete unwillingness to learn or to check what they repost. They had not heard of Hantaviruses before, and assume because they had not heard of it did not exist. Previous mentions therefore prove that this was a planned outbreak.
This is very much the same as their reaction to COVID-19. They had never heard of coronaviruses before. So we got memes featuring disinfectant labels from 2016 claiming to kill 99.9% of coronaviruses, with GOTCHA questions like “How did they know!!?” But there are many coronaviruses. They vary from very mild viruses which cause the common cold, to deadly variants like MERS and SARS. Anti-vaxxers didn’t know this, so they assumed that previous work on vaccines or cures was proof of a conspiracy.
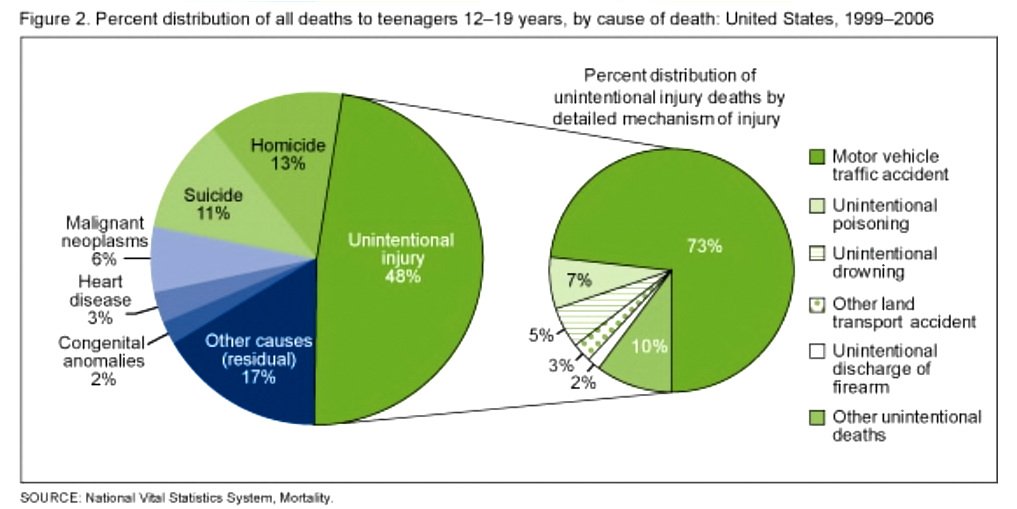
Similar ignorance-based fantasies relate to the claim that young people never died of sudden cardiac failure before COVID vaccines. But in the late 1990s and early 2000s, heart disease including sudden cardiac failure ranked fifth among leading causes of death for teenagers aged 12-19. The rate of sudden cardiac death amongst young people has slightly declined since then, including through the COVID period, because of better pre-sport testing, and the presence of AEDs at most gyms and sporting grounds.
In short, don’t be stressed about Hantaviruses, continue to ignore the arrogant and ignorant anti-vaxxers, and if you have questions or concerns about any disease or health related issues, talk to your GP or even better, a specialist in whatever field you are concerned about, eg a virologist or epidemiologist for viruses.
About twenty years ago a friend who had collapsed into new age silliness gave me a bundle of New Dawn magazines. She thought I would find them interesting. I did, but not for reasons she hoped.
Scattered through them was a series of articles she specifically asked me to read. These argued that Christianity had not existed before the Council of Nicaea.
What they claimed was that Constantine, aware that the Roman Empire was fracturing, had decided that a single, all-incorporating religion was key to re-unifying the empire. So he gathered religious leaders from around the empire, and charged them with creating a new faith that combined aspects of cults and religions from around the known world, and creating a prophet and scriptures to support this new faith. The name Jesus was fabricated from the names of the druid deity Hesus and the Indian god Krishna – Hesus Krishna became Jesus Christ. Constantine then mandated his new religion, and eventually the faked documents of the “New Testament” were assumed to be hundreds of years older than they were, and the faith of Hesus Krishna was claimed to have had its beginnings in an obscure Jewish prophet.
I had a brief email correspondence with the author. I pointed out that we have copies of large sections of the New testament, in documents like the Rylands Library Papyrus P52, and the Chester Beatty Papyri and Bodmer Papyri, some of which have been dated to 100AD to 150AD – 200 years before the Council of Nicaea. False, the author responded. Carbon dating doesn’t work. They are all forgeries. What about non-Christian authors like Josephus, Tacitus, Pliny the Younger, all of whom mention Jesus, with 100 years of the time he lived. Also fakes, responded the author. We live, he claimed, in a completely faked timeline.
But, I responded, we also know what happened at Nicaea, because we have multiple accounts from people who were there. Eusebius, Bishop of Caesarea, for example, who wrote a detailed description of the proceedings in his work Life of Constantine (Book III) and also wrote a personal letter to his church in Caesarea, explaining the reasons he had signed the Creed (mainly because the Creed expresses clearly what the Church had been taught from the beginning). Then there is Athanasius’ book Defence of the Nicene Definition. Athanasius was present at the Council. Eustathius of Antioch was there and wrote his own account of proceedings.
In addition there are letters written by Constantine before and after the Council. We know why the Council was called – to deal with claims by the priest Arius that Jesus was not fully divine, and we have widespread evidence of the conflict caused by those claims. And of course we have the actual documents agreed to at Nicaea. You can find translations of those here: https://oer.minotstateu.edu/projects/105SourceReader/documents-from-the-council-of-nicaea.html None of those documents show any attempt to create new scriptures, nor to invent a new religion.
All fakes, he replied. Constantine had a vested interested in creating a new religion, and was happy to pay to create fake documents to give it authenticity. Gosh. OK. But then what about the Early Church Fathers? I asked. “The what?”, he replied. The hundreds of Christian hymns, sermons, letters and books by bishops and teachers around the empire that come from before the Council. All fakes. They were just made up to give Constantine’s new religion background.
What evidence exists for what you are claiming? I asked. Are there letters or decrees from Constantine you can point to, or documents from members of the Council that support your claims? They have all been destroyed, he answered, to uphold the narrative.
So if all the documents have been destroyed, how did you come to your conclusions about this?
Some of the original documents are in the Secret Vatican Archives. Someone who works there was going to reveal all of this but died in a “car accident.”
The Secret Vatican Archives are not exactly secret, I replied. Almost any research scholar from any religious background or none can visit them. Thousands do every year. And what was the name of the employee who mysteriously died?
He gave up at this point. I have given you the evidence, he said, you decide if you want to believe it, or not. But of course he hadn’t given me any evidence.
The Council of Nicaea and Church history in general are all very interesting, but what has this got to do with Bill Gates?
The answer is that the foregoing is very much like arguing with anti-vaxxers.
Naomi Wolf, for example, is to science reporting what Michael Baigent (The Holy Blood and the Holy Grail) is to theology. Both she and Michael Baigent and his co-writers start with a “conspiracy theory” mindset, assuming something dramatic and nefarious is being hidden, and rely on innuendo and selective reading of records to arrive at conclusions they settled on in advance. In Wolf’s case her bizarre story-telling is compounded by the fact that seems to have not the most basic idea of what she is talking about. Very much like my “Constantine invented Jesus” friend.
For example, Wolf’s recent conclusion that NIH-funded research created SARS-CoV-2 and officials covered it up rests on a speculative leap from “NIH funded coronavirus research” to “NIH secretly created the pandemic virus” without any evidence that any NIH-funded experiment actually produced SARS-CoV-2. She assumes that NIH grants to EcoHealth Alliance, some of which were used to conduct research on coronaviruses, prove that that Anthony Fauci and the NIH were engaged in creating a bio-weapon. But she provides no DNA sequence data, lab records, or primary scientific evidence, or any evidence at all linking any NIH funded research to the pandemic virus.
She doesn’t appear to understand how NIH grant oversight actually works. She treats ordinary grant documentation as evidence of secrecy or malfeasance, when in reality NIH grants undergo peer review, ethics oversight, and public reporting requirements. Anthony Fauci has no personal involvement in the grant process, nor any role in approving which applications are approved. She ignores or is not aware that thousands of NIH grants support basic virology research worldwide, including coronaviruses.
She seems confused about what “gain-of-function” is, and uses it as a blanket term for any coronavirus research. The regulatory definition doesn’t mean this at all. It means specific research into how viruses adapt and change to enhance their transmissibility or virulence. By collapsing this distinction, she treats ordinary grant-terms and policy-compliant research as if it were prohibited or dangerous or inherently nefarious.
Gain of function research is important because it gives us key insights into how viruses may adapt to spread to humans, or may become more dangerous. This process goes on all the time in nature. There are jumps from animal or bird only viruses to human. Ebola, MERS and Zika and are just few recent examples. Gain of function research is not about creating biological weapons, but about helping us prepare for those changes when they occur.
Wolf does not seem to understand statistics or science administration, or even to have a basic grasp of science. Her money-making success and the reposting of her claims relies on the fact that her readers and listeners are similarly impaired, just as John M Allegro relied on the ignorance of Biblical languages of the feverish mob who bought his book The Sacred Mushroom and the Cross, or Hugh Schonfield relied on the lack of knowledge of his readers of ancient and Biblical history for his best-selling book The Passover Plot.
She has professional sounding supporters, of course. William Makis, oncologist and cancer researcher. Except he was found guilty of unprofessional conduct in 2018, is not licensed or registered to practice medicine anywhere, and was a radiologist, not an oncologist. He has never conducted any cancer research. Robert Malone, the creator of mRNA technology. Except he was not the creator of anything. He was a secondary author on three papers published in 1989, 1990 and 1993, and has written nothing since. His claims are regarded as laughable by people who really did work on the development of the use of mRNA in medicine.
People who believe in Bible and history conspiracy theories believe they have experts on their side. John M Allegro, for example, was a respected University of Manchester academic, highly regarded for his work on the Dead Sea Scrolls. Hugh Schonfield was also a respected Biblical scholar with a doctorate from Hebrew Union College. But in any university or seminary around the world anyone who said they were a fan of either would find people looking at them in alarmed confusion before smiling and backing away slowly.
Ditto for people with any knowledge of science when someone says they are a fan of people like Naomi Wolf or Judi Mikovits. I have written about the egregious Miss Wolf (I cannot call her Dr) before, and will not repeat the comments made there: https://qohel.com/2024/10/23/naomi-wolf-and-the-pfizer-papers/
Judi Mikovits is a former, now unemployable, lab assistant, whose claim to fame was that she “discovered” that DNA from xenotropic murine leukemia virus–related virus (XMRV), a mouse‑related retrovirus, could be detected in many patients with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) but not in healthy controls. The original paper was published in Science in 2009. Science not only retracted that paper but also investigated concerns about image manipulation and data integrity in that and related work.
A detailed review in a medical journal describes her as a “serial scientific fantasist” whose published XMRV evidence was “unequivocally shown” to arise from contamination and explicit fabrication, and notes that she was never a leading figure in retrovirology prior to the XMRV episode. More information on the mendacious Miss Mikovits here: https://pmc.ncbi.nlm.nih.gov/articles/PMC7398426/
But what about Peter McCulloch? You can’t deny that he was a respected cardiologist. No, that’s right. He WAS a respected cardiologist. Just Like John M Allegro and Hugh Schonfield WERE respected academics. Now he makes a fortune selling fake cures to cancer victims. His company, the Wellness Company, sells multivitamins, “spike detox” supplements, and pricier “adverse‑reaction” packages (typically hundreds of dollars) aimed at people who believe they were harmed by vaccines, including people suffering from cancer. Commentators in public‑health and science‑communication circles have described this as a scam. McCulloch promotes dramatic, disproven claims about vaccine “spike” danger, then directs people toward expensive supplements that he and his company profit from, all without evidence that these products treat or prevent anything real.
A couple of articles here on the no-longer-licensed-to practice-medicine-anywhere Dr McCulloch:
Alternatively, if you are interested in reality, you could actually read some actual scientific research by actual scientists, a very small part of which is summarised here, with links to original papers:
Of course anti-vaxxers will continue to shriek “It’s all paid for by big pharma!!!” But that is just something anti-vaxxers say. They can’t produce any evidence of this because there isn’t any evidence, any more than religious nuts can produce evidence that Constantine invented Christianity. In reality research funding comes from multiple government, private and commercial sources.
When your faith in what you see on social media demands that you believe that almost all doctors, nurses, universities and government health departments around the world are corrupt and care more about money than their patients, and that fake scholars like Wolf and Mikovits or the one in 100,000 medical personnel who are grifters like Makis and McCulloch who make a fortune out fake cures are really the ones who are really bravely telling the truth, then you either need to do some serious reading and thinking, or you need to consider whether such a baseless and paranoid way of looking at the world and the people in it is so divorced from reality that it amounts to mental illness.